
Read Part 5 >>
CITY VIEW HOSPITAL INITIATIVES
The hospital administration was aware of the dispersal of the community, of its aging staff, and of its decreased name recognition. It did try to recruit younger physicians onto its staff and attempted various other approaches towards building up its clientele. It could do little to change the dispersal of the community, but perhaps it could redefine its mission within the community in ways that would ensure its survival in coming years.
The non-profit corporation known as “Memorial Hospital of the Japanese Community” was solely embodied by City View Hospital at its incorporation in June, 1961. But the articles of incorporation also allowed the corporation “(t)o establish, maintain, conduct and operate hospitals, sanitaria, asylums, rest or retirement homes . . . ”1 Therefore, eight years after the move of the hospital to City View, the “Memorial Hospital” corporation expanded its services by opening the Keiro nursing home near the hospital, in 1969. How did the impetus of this expansion arise?
By the latter half of the 1960’s, City View had begun to run into the problems involved with placing Japanese-speaking patients into nursing homes. The hospital decided to carry out a needs survey to assess whether there was a significant need within the Nikkei community for a nursing home. The study confirmed that a nursing home was needed. Therefore, trustees of the corporation took steps to establish the first Japanese nursing home, by soliciting funds from the community. The Nikkei community gave the trustees strong financial support and the nursing home was promptly established. The nursing home was named “Keiro” which means “respect the elderly” in Japanese.
The new nursing home quickly developed a long waiting list. Evidently, the need for nursing home care was much greater than expected, with applications originating from the Midwest, East Coast and West Coast of the U.S. So in 1974, the Minami Keiro nursing home was added, also near the hospital, followed by the Japanese Retirement home in Boyle Heights in 1975 and the South Bay Keiro Nursing home in 1981 in Gardena.2
Whether by design or by circumstance, Memorial Hospital of the Japanese Community Corporation now consisted of five facilities, four nursing homes and City View Hospital. Given that the hospital had discontinued its obstetrical services by 1976 while serving greater numbers of elderly patients in its nursing homes, the purpose of the corporation shifted towards caring for elderly Japanese-Americans.
The five facilities constituted the “Umbrella of Care.” With this “umbrella” the corporation was now well equipped to serve the elderly Japanese-Americans that the Nikkei community had left in its care. Unfortunately, this heavy dependence on the elderly Japanese-American patients would leave the hospital itself vulnerable. For a new U.S president had taken office, with a health policy agenda that would eventually lead to the demise of City View Hospital.
City View embarked on another initiative which expanded its role into health education. With the premier May 1983 issue of the VIEWS newsletter, City View inaugurated its Family Health Program.3 This program based itself on the opinion that the key to a healthy community lay in promoting healthily functioning families that were as medically informed as possible. The newsletters were made available to the community through the five facilities, and through contacts gained in the course of the fundraising campaigns for each facility. They contained current general medical information from staff consultants, ideas for family activities, and announcements of special health events, which included activities ranging from conferences on health issues to family nights at sport events. The conferences and the newsletter VIEWS were both well accepted, and in regard to the conferences, well attended.
By 1985, the corporation was functioning well in its newly defined roles, and had overcome some of the problems it would have faced had it remained tied to its old role of a community hospital. Instead, the Memorial Hospital corporation now oversaw an “Umbrella of Care” health care system, focusing on the health care of elderly Japanese-Americans. And, although it had sacrificed its obstetrical care and had fewer pediatric patients, it was beginning to reestablish contact with families via its health education newsletter and conferences. Given time, it may well have been able top make progress on building up its patient referrals again, for it planned to start an intensive care unit soon. But time had run out.
DRG’S AND THE FINANCIAL CRISES
Starting with its 1982-83 fiscal year, City View Hospial was required by the federal government to begin using the “Diagnosis Related Groups” (DRG’s) system of funding. Certain features of these DRG’s worked against the health of the hospital’s finances. First of all, the DRG’s paid a predetermined amount of money for a given diagnosis that was not adjustable for the severity of a given hospitalization. Also, only one primary diagnosis per admission was allowed. Both of these features worked against City View, in that over 70% of its patients were over 75 years of age, and had longer stays and more complicated illnesses than the population on which the DRG’s were based. Therefore, the money which the DRG’s provided was not sufficient to cover patient care costs.
A third feature of the DRG’s was adverse to City View, in that they were adjusted to account for the amount the hospital had charged previously. Apparently, City View had historically operated very efficiently in the past. This past efficiency was now a liability to the hospital, for its compensation was accordingly downward, compared to another hospital that might have previously operated inefficiently and therefore had more compensation, and more reason to streamline itself in the future. This was a particularly untimely feature, since City View had just started its intensive care unit the previous year, which was not early enough to affect this rate of compensation.
_____________________________________________________________
Admissions Data for City View Hospital, 1979 to 1983
taken from data provided by the hospital records department.
Fiscal years
beginning November 1st 1983 1982 1981 1980 1979
Average daily census 9.9 12 10.5 11.8 13.3
Percent occupancy rate 18.70% 22.60% 19.80% 22.30% 25.10%
# patient days for patients
> 75 years old 1772 2758 2388 2410 2868
65 to 74 years old 661 559 477 550 695
< 65 years old 1181 1069 981 1374 1311
Percent of patient's days
covered by Medicare 83% 76% 75% -- --
Percentage of total patient days
accounted for by patients
> 75 years old 49% 63% 62% 56% 59%
Percentage of total patient days
accounted for by patients
> 65 years old 67% 76% 74% 68% 73%
_____________________________________________________________
The financial data in the accompanying table shows the impact that the DRG’s had on hospital operations. From 1981 to 1982, total operating expenses had risen by 1.2 million dollars, mainly as a result of starting the intensive care unit. Gross patient revenue had also risen by 1.5 million dollars as a result of the new unit. But the new system of DRG’s increased the amount of deductions from the gross patient revenue by 1.9 dollars, explaining in large part the hospital’s loss of $905,234 for the year. And in the following fiscal year, starting in November 1983, City View registered a loss of $569,606, again accounted for in large part by the increased deductions from gross patient revenue resulting from the new system of DRG’s.
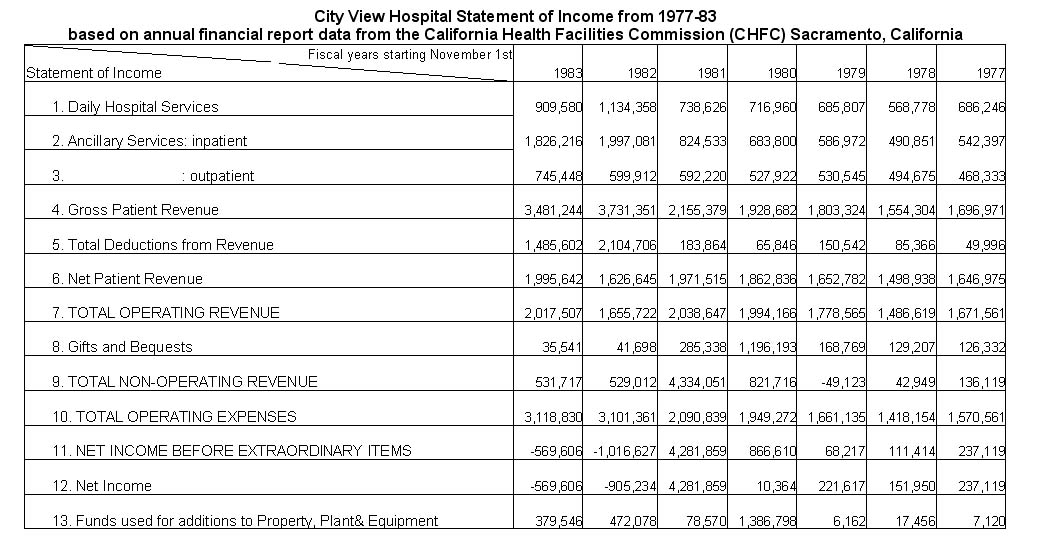
City View Hospital Statement of Income from 1977 - 83. Click to enlarge
Notes:
1. Articles of Incorporation, Memorial Hospital of the Japanese Community, July 19, 1961, Corporate Division, Secretary of State, Sacramento.
2. Personal conversation with Edwin Hiroto, September 4, 1985.
3. VIEWS, May 1983 Issue.
© 1986 Troy Tashiro Kaji

